
Yesterday, we drove out to UPenn in Philadelphia to meet with Dr. Loren. We hadn’t seen her since March and we were hungry for information and for some kind of timeline for the transplant.
Well, we did get a lot of information. Some of it good, and some of it rather daunting.
GOOD NEWS: Dr. Loren said that George looked great! She was very pleased with his physical and mental states. She also said they had located several donors in the National Bone Marrow Registry (NBMR) that are perfect matches for George! Of course, one of those matches could be George himself because he participated in a bone marrow drive years ago for a military member so he is in the registry! Ugh. She said she and her team had been waiting for this appointment to get an “eyes on” assessment of George before making decisions for treatment and moving forward.
DAUNTING NEWS: Before the transplant, George will undergo “conditioning” treatment to get his bone marrow and body ready for the new marrow. There are two different approaches to this treatment. One is the “myeloablative” conditioning. This is high intensity chemotherapy with radiation. The intent it to completely wipe out the bone marrow and takes a scorched earth approach to it. The other approach is to use a reduced intensity conditioning. It’s a less strong chemotherapy regiment and no radiation. Because the majority of people diagnosed with AML are over 65, many of the patients can’t handle the myeloablative conditioning, they devised this less intense regiment.
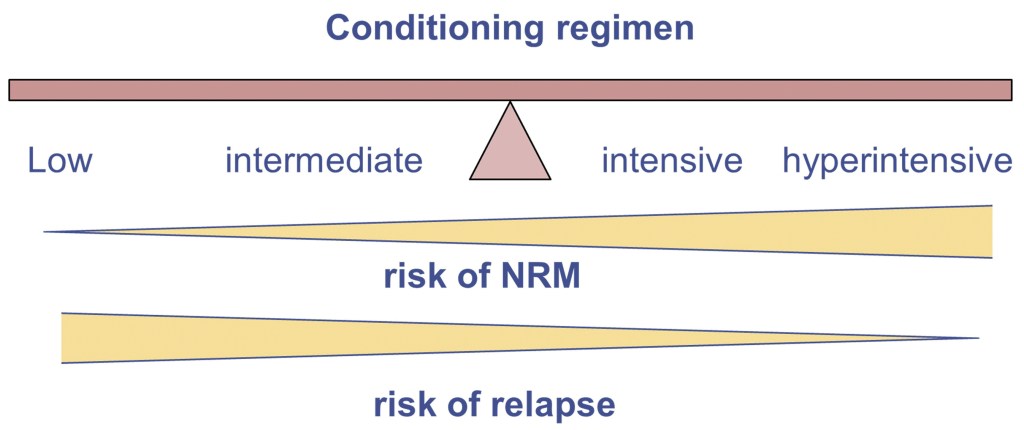
In the illustration above, you can see the benefits and the disadvantages of each conditioning regiment. While the hyperintensive (myeloablative) treatment has a much lower risk of relapse, it also has a higher risk of NRM (non-relapse mortality). The risk of GvHD (graft vs host disease) is higher, as well as other infections that could be contracted while the body is undergoing the chemo. This chemo completely wipes out your bone marrow and therefore, your immune system is shot. That makes you vulnerable to deadly infections. However, the less intense chemotherapy has a higher risk of relapse. How devastating to go through all this pain, uncertainty, fear and disruption in your life only to have the leukemia come back, which it can do as early as three to six months after transplant!
So, Dr. Loren said she is leaning towards the myeloablative option for George for a few reasons. First, because George is relatively young (yes, you are considered young in the leukemia world if you are under 60!) and in relatively good health, she believes his body can take the stronger chemo and radiation. This was part of the reason she wanted to get an eyes-on assessment of him. Secondly, after George’s first round of chemo right after his diagnosis (induction chemo) they did a bone marrow biopsy and while they found him to be technically in remission (he had less than 5% myeloblasts in his marrow), the cellular mutations that increase the risk for relapse were still detected, so she feels like his leukemia “seems to be a stubborn one” and requires a stronger approach. Thirdly, our goal is a CURE, not just remission. We do NOT want a relapse. We want to tackle this thing head on, defeat it and come out on the other side able to resume our beautiful life together without having to constantly worry about relapse. Now, don’t get me wrong. Relapse is always a possibility, but the high intensity approach decreases the chances. We also don’t want to have to go through the transplant process again. The high intensity chemo can cause damage to your heart, organs, eyes, etc and you DO NOT want to do it more than once!
George and I agree with Dr. Loren. So, the myeloablative conditioning it will be. His next step is to schedule his pulmonary function test and transthoracic echocardiogram appointments so he can get cleared for the chemo.
Dr. Loren was very frank and talked about a lot of real stuff. Like the fact that some patients actually die during the conditioning treatment from infections. That some patients die from GvHD (like rejection from an organ transplant) after the transplant, although that number is very low. That relapse can happen, which actually was kind of a surprise to us because we had been told that the transplant was a cure. We had in our minds that cure meant DONE. Apparently not.
George asked where on his body they would use radiation…would it be his pelvic area where the bone marrow is? Ummmm…..NO. It is Total Body Irradiation (TBI), meaning he lies on a table twice a day for three days and they radiate his entire body. This is done to: 1) destroy cancer cells in areas where chemotherapy can’t easily reach (such as your nervous system, bones, skin, or testes), 2) decrease the response of your immune system. If you’re having an allogeneic stem cell transplant (getting bone marrow or stem cells from a donor), your body may see the cells as foreign. If this happens, your immune system will try to destroy them. Having TBI before your transplant can help keep this from happening and 3) to create space for new bone marrow to grow (engraft).
Dr. Loren told us most people hurry up and wait….with the transplant process it’s wait, then hurry up. We are waiting now for the matched donors to be contacted, to determine if they are healthy and willing to donate to George. Meanwhile, she suggested no more chemo until we get a better idea of the timeline. Once a donor is contacted and vetted, things could move quickly. She estimates it will be 4-8 weeks until transplant. George has his next appointment with Dr. Loren on June 1.
We are scared, but excited at the same time to move forward with the transplant. The truth is, we don’t really have a choice.
Dr. Loren told George he can travel – even to Europe! Once his white cell count comes up, of course. I was excited, thinking we could fit a trip to Greece in before everything starts happening. But then George reminded me that he could be really sick and unable to work during the transplant process and he needs to save his vacation days because…well, capitalism. His sick days never expire, but his annual vacation days are use or lose. Sigh. We will definitely take a couple of weekend jaunts out to the Hudson Valley or the Poconos though!

Leave a comment